

Background:
Treatment options for relapse after allo-SCT remain limited with poor outcomes. Second Allo-SCT provides benefit to a small subset of patients (pts). However, relapse rates after second Allo-SCT are high and novel approaches to improve outcomes after second Allo-SCT are needed. Conventional total body irradiation (TBI) can reduce relapse rates, but greater radiation doses cannot be delivered safely without increasing the toxicity to surrounding normal tissues and organs. Total marrow irradiation (TMI) techniques permit dose escalation while substantially reducing doses delivered to normal tissues relative to conventional TBI. We conducted a phase I study to assess the feasibility of combining TMI with a fludarabine-melphalan conditioning regimen for second or beyond Allo-SCT to decrease relapse.
Methods:
Inclusion criteria required a matched/mismatched donor and relapse after previous allo-SCT. GVHD prophylaxis was tacrolimus and mycophenolate mofetil, plus ATG for mismatched donors (NCT02333162). From December 2015 to May 2020, twenty-two pts with were consented to this 3 + 3 phase I trial design; one pt failed to proceed and was replaced. 21 pts (18 AML, 2 MDS/MPN, one ALL) were treated with linac-based volumetric modulated arc therapy (VMAT) technique using 6 MV photons. TMI was provided twice daily at 1.5 Gy per fraction starting with a total dose of 6 Gy, with dose escalation to 9 Gy and 12 Gy. Mucositis was an adverse event of special interest and assessed by the WHO Mucositis Score on days 7, 14, 21, and 28 post-transplant to investigate the combined mucosal injury from alkylating chemotherapy and radiation.
Results:
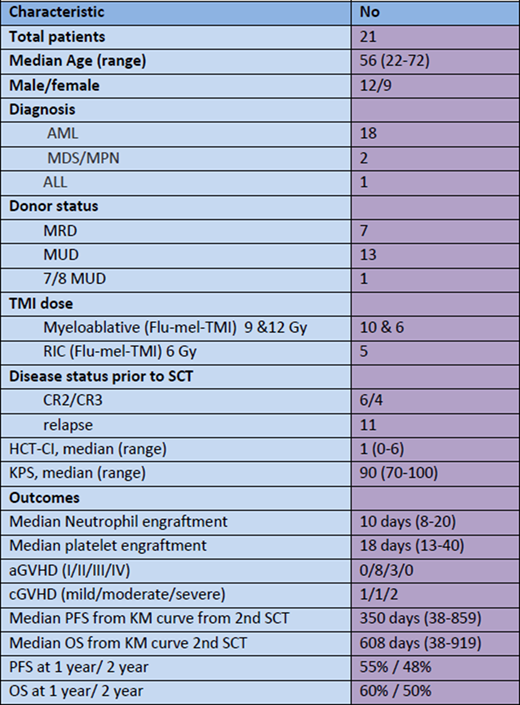
Baseline characteristics are summarized in Table 1. The median age was 56 years. All had matched donors except for one mismatched unrelated donor. 6 pts were in CR2, 4 pts in CR3, and 11 pts had refractory disease prior to 2nd SCT. 3 pts treated on dose level 6 Gy had no DLTs. At dose level 2 (9 Gy), the first pt of the cohort of six pts had grade 3 mucositis as a DLT on day 7; it resolved by day 21. The first 2 pts at dose level 3 (12 Gy) had no DLT, but the 3rd pt had DLT of grade 3 mucositis on day 7, resolving by day 14. Two more pts were treated and none had DLT. A sixth pt with refractory disease was treated but had graft failure with concurrent bacterial, fungal, and viral infections. This pt also developed grade 3 mucositis on day 14 that progressed to grade 4 on day 21 but resolved by day 28. Thus, we determined the MTD for TMI was 12 Gy; 9 Gy was an alternative dose for less fit or older pts.
SCT outcomes were listed in Table 1. As mentioned above, 1 pt had primary graft failure, and one pt failed to have platelet engraftment due to early relapse. 11 pts developed aGVHD with cumulative aGVHD at 58%, and 4 pts developed cGVHD with cumulative cGVHD at 33%. With median follow up of 11 months (1 - 30 months), 6 pts had disease relapse after a median of 205 days (46-464 days); 10 pts have died (5 from PD; 2 from infection, 1 from GVHD, 1 from PTLD, 1 from second malignancy). Two year PFS and OS were 48% and 50% respectively, which compare favorably to the 2 years PFS and OS of 17.5% and 22.6% from our historical data with 65 pts who had 2nd Allo-SCT prior to this TMI trial at our center (Fan et al. Exp Hematol Oncol 2019).
Conclusion:
We recommend 12 Gy of VMAT-TMI as the MTD combined with fludarabine-melphalan (140mg/m2) as a conditioning regimen for second allo-SCT. Grade 3-4 mucositis was transient, peaking at days 7-14, and resolving by day 21-28. 9 Gy may be appropriate for less fit or older pts. The 2 year PFS and OS of 48% and 50% after second Allo-SCT for this novel TMI-based regimen are sufficiently encouraging to warrant further study.
Liu:Agios: Honoraria, Other: Regional Advisory board meeting; BMS: Research Funding; Karyopharm: Research Funding. Stock:Pfizer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Research to Practice: Honoraria; Jazz Pharmaceuticals: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Membership on an entity's Board of Directors or advisory committees; Kite: Consultancy, Membership on an entity's Board of Directors or advisory committees; Agios: Consultancy, Membership on an entity's Board of Directors or advisory committees; Morphosys: Consultancy, Membership on an entity's Board of Directors or advisory committees; Abbvie: Honoraria, Research Funding; Novartis: Research Funding; Leukemia and Lymphoma Society: Research Funding; American Society of Hematology: Honoraria; Adaptive Biotechnologies: Consultancy, Membership on an entity's Board of Directors or advisory committees; UpToDate: Honoraria; Servier: Consultancy, Membership on an entity's Board of Directors or advisory committees. Larson:Novartis, Takeda, CVS/Caremark, Celgene, Amgen, Epizyme: Consultancy; Astellas, Celgene, Daiichi Sankyo, Novartis, Rafael Pharmaceuticals, Cellectis, Forty Seven: Research Funding. Kline:Verastem: Membership on an entity's Board of Directors or advisory committees, Research Funding; Kite/Gilead: Speakers Bureau; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees; Karyopharm: Membership on an entity's Board of Directors or advisory committees; Merck: Research Funding. Riedell:Novartis: Consultancy, Honoraria, Research Funding; Kite Pharmaceuticals/Gilead: Honoraria, Research Funding; Bayer: Honoraria; Celgene/Bristol-Myers Squibb Company: Honoraria, Research Funding; Verastem Oncology: Honoraria; Morphosys: Research Funding; Karyopharm Therapeutics: Honoraria. Bishop:Novartis: Membership on an entity's Board of Directors or advisory committees, Research Funding; Autolus: Membership on an entity's Board of Directors or advisory committees; BMS: Honoraria, Speakers Bureau; CRSPPR Therapeutics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Kite: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Incyte: Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal